In 1984, I founded the Center for Development Communication (CDC) as a private, not for profit professional organization. This page will cover the “Sehettak Biddonia” project, which was CDC’s first project, and indeed the one which CDC was originally established to implement.
Why did I have to establish CDC?
When I developed the “Sehettak Biddonia” concept, there was no institution in Egypt at the time that could provide the enabling environment to implement the project, which was based on the idea of integrating communication theory, research and creative production. I decided therefore to found CDC in order to create the needed structure and enabling environment that would make it possible to develop and implement this pioneering project.
The donors of Sehettak Biddonia encouraged this step and I therefore wish to thank them because it would have been virtually impossible to bring this project to life without CDC.
Before going into more details on this topic, let me quickly alert the reader that CDC didn’t stop at the Sehettak Biddonia project. In fact, CDC has quickly become the major organization in Egypt and the Middle East for developing and implementing social marketing and communication for development campaigns. For more on CDC’s projects, please see:
https://elkamel.wordpress.com/category/health-population/
https://elkamel.wordpress.com/category/the-environment/
https://www.youtube.com/channel/UC5tP8ymfMVivlZnZ1Tp9L3g
“Sehettak Biddonia”
“Sehettak Biddonia” means in Arabic (Your Health is Worth the Whole World). It’s also the name of a project that was developed by Dr. Farag Elkamel and submitted as an unsolicited proposal to Johns Hopkins University, Unicef and the Ford Foundation in a pioneer and comprehensive initiative to define and test the media potential for the prevention of various health problems in Egypt. The Canadian International Development and Research Center (IDRC) also joined as a fourth donor at a later stage.
The main justification for the need of this project was the fact that Egypt had several health challenges that could be prevented with good communication. However, whatever was being done in this respect could be classified as no more than paying lip service to the cause. Health programs on radio and TV were quite boring, and the few public service announcements that were produced by the ministry of health lacked the basic principles of effectiveness.
On the other hand, 50 percent of all Egyptians, including 70 percent of all adult women were illiterate at the time this concept was developed, while, 93 percent of them had access to television and watched it on a regular basis. TV therefore had the promise to become the “knowledge-leveler”, overcome the illiteracy hurdle and provide the badly needed health information to all citizens.
But the challenge however was the contaminated health communication scene in Egypt, where bad quality health messages were disseminated with virtually no effect. The argument then became like this: how can we develop the needed health messages and present them to those who desperately need them, and in the most effective ways.
Positive feedback and evaluation reports about the TV campaign which I developed for the Oral Rehydration Therapy (ORT) project had become available, which encouraged donors to support the concept and express their willingness to fund my proposal.
Work on the project began on April 1, 1985. As planned, the project started with extensive research on the general public and public health professionals, and invited Egyptian and expatriate health experts to attend a major conference in order to discuss the project concept, plans, as well as message selection and prioritization. The project’s stated objectives were as follows:
- Upgrade Egyptian quality of life through dissemination of essential health information.
- Demonstrate the force of sound social research, coupled with modern communication techniques to improve social problems such as lack of health education.
- Prove the usefulness and effectiveness of television in this type of social development communication.
Project Phases
The Sehettak Biddonia project was divided into four phases: 1) research, 2) planning and message development, 3) production and pretesting of pilot messages, and 4) production of TV spots and soap opera.
Phase One: Research
The following research was conducted:
- A literature review of printed media to determine the attitude of government officials, media personnel and the general public towards using public channels to disseminate health information.
- A survey of 100 Egyptian physicians to determine what the public should know in order to more easily communicate with doctors. The sample included directors of MOH semi-autonomous projects and public health professors at universities in the greater Cairo metropolitan area.
- A survey of 20 national and international social scientists concerning the social, anthropological, and economic aspects of Egyptian health problems.
- A survey of 900 mothers in 9 different governorates to pinpoint their knowledge, attitude and understanding of specific health problems. A cluster sampling method was used in rural and urban sections of the country both in the Delta (Cairo and Alexandria) and in Upper Egypt. A questionnaire consisting of 99 questions was used to collect essential data on media and health practices.
- A survey of earlier health education and communication projects in Egypt and other countries to develop guidelines from successful programs.
- Compilation of recommendations from attendees at a CDC Media and Health Education Conference held in Ismailia, Egypt, January 10 and 11, 1986, concerning health education priorities in Egypt, health priorities for child survival, target audience composition, message content, and the media’s role in disseminating health information
Phase Two: Planning, Concept and Message Development
Phase Two of the Sehettak Biddonia project called for prioritizing Egypt’s health problems and developing media concepts and approaches. A list of 156 priority health issues was developed from the following:
- “Health Profile of Egypt”, a survey conducted by the Ministry of Health;
- The “Elite Doctors’ Perspectives on Egypt’s Health Problems”,
- The “Highlights of Mothers’ Knowledge, Attitudes and Practices Survey on Basic Child Survival Communication Issues”,
- The “Media and Health Education Conference Recommendations”,
- Various reports obtained from the Ministry of Health concerning the types and number of emergency service required,
- A report from the Central Agency for Public Mobilization and Statistics listing health statistics such as causes of death, types of hospital services requested types of diseases reported and maternal-child health problems.
A script writer’s guide to these 156 issues was created in both Arabic and English. It breaks down major points such as nutrition into specific topics, e.g., nutrition for pregnant women, child nutrition during weaning and illnesses, and recognition of malnutrition in a child, and lists the relevant socio-cultural background information and the message that should reach the target audience. The validity of each technical point was tested through focus group research at the local level and personal interviews with top health professionals both from the Ministry of Health and major faculties of medicine. As results and comments returned, they were analyzed and revisions were made.
As health issues were being determined, CDC developed an overall media concept and approach:
- Target audience – composed of adult men and women residing in urban and rural areas. Special attention will be paid to making messages simple enough to be understood by rural and illiterate audiences.
- Message guidelines – regardless of content, all messages will be medically correct, culturally relevant, actionable, based on research, and presented in a clear, simple and interesting manner.
- Language and visuals – all messages will use the standard Egyptian dialect and words will be comprehensible to all segments of the target audience. Visuals will reflect the typical physical environment of the main segment of the target audience.
- Tone and approach – all messages will use a positive or neutral tone. Characters will be representative of corresponding target audiences.
- Program format – The Sehettak Biddonia programs will have two formats, both of which rely on the elements of drama and entertainment: short (1-2 minutes) commercial-type messages and a long social dram consisting of 15 episodes each of which is 45 minutes long. The episodes will also incorporates songs and folk elements.
- Framework and themes – although the spots and the drama will have essentially different formats and themes, each will attempt to contain elements of the other to reinforce the message.
- Dissemination – all Sehettak Biddonia messages will be aired during prime viewing time.
- Pretesting – messages will be pretested among target group members and results will feed back into program re-planning and shortcomings will be accordingly adjusted.
Phase Three: Production and Pretesting of pilot messages.
In March 1987, the project’s third phase was completed: production of pilot messages. Those issues designated for immediate coverage in the first series of spot commercials are immunization, birth spacing concepts, early weaning, Tetanus Toxoid and bilharzias. They were partly selected to coincide with Egypt’s 1987 Year of the Child campaign. The remaining topics will be covered in the future as funding becomes available.
Phase Four: Final Production and Dissemination
The output of the project included a TV drama series, “The Family House” and 10 TV spots. With partial support, CDC went ahead and produced a second part of the series with the name “Bread and Salt”, which also carried health and environmental messages. All of these productions were aired free during prime time on Egyptian TV.
Before going into a detailed description of these phases, let me jump to the output of this project, and briefly present the two major outputs: the TV Spots and the Soap Opera.
TV Spots
The television spots addressed various health issues, including child spacing, immunization against measles, polio, and tetanus during pregnancy. The spots also addressed correct weaning practices, schistosomiasis prevention and treatment, in addition to female genital mutilation (FGM).
This pioneer experience has succeeded in developing the appropriate methodology for using TV in health campaigns in Egypt, and has also paved the way for getting free airtime for public service announcements in Egypt.
The 10 spots mentioned above can be viewed (with English subtitles) here:
The Soap Opera
As indicated above, a major component of this project was the development and production of an entertainment-education soap opera to test the potential of this format for addressing deep-rooted health and social beliefs and practices. This innovative project consisted of conducting necessary audience research in three countries (Egypt, Jordan, and Morocco), as well as developing, producing and distributing a 12-hour television drama series consisting of 15 episodes.
In addition to addressing the issues of family planning and early marriage, the “Family House” carries essential messages on AIDS awareness and prevention, environmental protection, acute respiratory infections (ARI), home accidents, and drug addiction. The series has been aired in Egypt, Morocco, and Lebanon. It has been watched by over 90 percent of all adult television viewers in Egypt, and more than 80 percent of them liked it and learned from it. Other parts of this site address this series in more details, but here is link to the series itself:
The Mothers’ KAP Survey On Basic Child Survival Communication Issues
Highlights of Mothers’ KAP Survey On Basic Child Survival Communication Issues
By: Dr. Farag Elkamel
January 5, 1986

The Center for Development Communication (CDC) carried out a survey of 900 mothers of children who are less than three years of age in nine governorates. The survey was conducted from July through September 1985, and employed the cluster sampling technique. The survey instrument used was a questionnaire containing a total of 99 closed and open-ended questions. The nine governorates where the survey took place are: Cairo, Behera, Dakahlia, Sharkia, Gharbia, Suhag, Kena, Menya and Assuit. Unicef, Johns Hopkins University, IDRC and the Ford Foundation sponsored the study as part of the Sehettak Biddonia project. The purpose of the study was to establish a baseline and uncover the priority health issues and messages to be addressed by this pioneering project.
Major health issues covered in the survey are breastfeeding, weaning foods and practices, immunization, mother and child nutrition, diarrhea and dehydration, acute respiratory infections, child spacing and family planning, home sanitation, food and personal hygiene, and water supply and sewage.
A. Breastfeeding
Of the total sample of 900 mothers of children under three years of age, 85.6% reported breastfeeding their children. A greater percentage is expected for mothers of children less than two years old. The majority (84%) of breastfeeding mothers said that they breastfeed their babies at night, too.
For those who said that they did not breastfeed their children, the number one reason given by 8.6% of the total sample was that they did not have enough milk. Other reasons given were that the mother is sick (1.9%) and that the child is sick (1.2%). While 21 mothers gave other various reasons, only one mother reported not breastfeeding because she preferred the artificial formula, and only five mothers said that they did not breastfeed because they could not stay at home.
When mothers were asked about the substitute they gave their infants, the majority of those who did not breastfeed said that they gave powdered milk (12.7% of total sample). The remaining mothers gave cow and buffalo milk (1.8%).
The majority of mothers who artificially fed their children consulted a physician (12%). The remaining 2.8% consulted relatives and other people. The vast majority of mothers who are not breastfeeding their children use other substances while the child was very young. Half of the mothers substituted breast milk during the baby’s first month and the other half during the second and third months.
Almost all mothers who are not breastfeeding use the bottle rather than other mechanisms such as a glass and spoon. Nearly half of those giving bottled milk have only one bottle at home, and most of the remaining half have two bottles. Almost all women using the bottle said that they threw away milk remaining in the bottle after feeding their babies.
B. Weaning Practices
Half of the women in the study sample of 900 cases reported weaning their babies before the 24th month. A vast majority of the remaining 50% mothers (44%) said that they weaned their babies exactly when the babies became two years old.
Egyptian mothers practice a gradual rather than sudden weaning process. More than three-fourths (76%) of mothers in the sample said that they gave their children other foods “Talhees” while milk feeding them. Before the child is one year old, almost all mothers give supplementary feeding. In fact, more than half do so before the child is six months old. When asked about the first thing they gave their children, the most often mentioned foods were boiled potatoes, boiled rice, biscuits, beans, egg yolks, yogurt, and milk pudding (mehallabia.)
C. Immunization
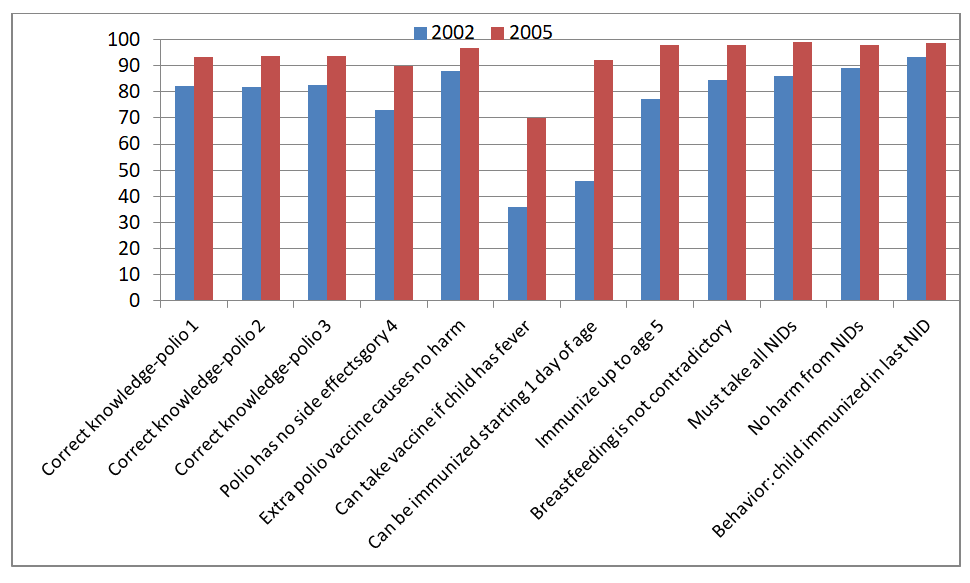
When the women were asked whether they had their children vaccinated or not, 87% said that they had done so and only 13% said that they had not. However, when they were asked to list the vaccines their children got, 83% of the entire sample said that their child was vaccinated against polio, 26%vaccinated mentioned tuberculosis, 40% mentioned measles vaccines, and about 10% said their children received a DPT vaccine. Interestingly, 16% of the women interviewed named non-immunizable diseases as ones that their children were inoculated against!
The great lack of information among mothers becomes more evident in their responses to a question on the number of times children should get immunized during the first year of life. Ten people said the child should receive a total of one vaccination, 33 mothers said they should receive two vaccinations, 255 women said three, 133 women said four, 107 women said five, 88 mothers said six times, and 68 mothers said seven or more times. One hundred and ninety-six women had no idea. Other more detailed information in the study reveals the wide knowledge gap between what the public knows and what they should know.
It is clear that the television polio campaign tremendously increased awareness about polio vaccinations. Of the total sample, 99% have heard of polio, and 67% of them heard of it from television. Twelve percent heard from health units, 9% heard via loudspeakers, 6% heard of it from neighbors and relatives, and the remaining 6% heard from other sources.
While awareness of polio vaccine was found to be extremely high, other aspects of knowledge about it were not the same. When respondents were asked about age at which a child should get the first polio dose, 175 mothers said two months, 337 said 3 months, 144 said four months, 28 said five months, 84 said 6 months, 80 people said more than 6 months and 52 people said they did not know.
In contrast with polio awareness, awareness of D.P.T. was quite low. Only 15% of the entire sample heard of D.P.T., and only a little over half of them (9% of total sample) know that D.P.T. is to be given three times, and almost the same number knew what the three D.P.T. diseases are.
Of the mothers surveyed, 61.7% said that their children had measles before. This is almost the same percentage of children who did not get the measles vaccine. The main reasons mothers mentioned for not having their children immunized against measles are that the child is too young, vaccines are unavailable, or that mothers do not usually know immunization sites and schedules unless they are announced via loudspeakers.
It is significant that when asked how to protect their children from getting the measles, only 217 mothers answered ‘by vaccination’. Two hundred and thirty-one said nothing could be done, 183 said they did not know, and the rest stated different opinions.
Unfortunately, 31% of mothers said that they would let their healthy children get near a child infected with measles so that they would catch it too. Ninety-seven mothers said that the reason was that they wanted to care for all of their children at once, 54 women said that they would do this because sooner or later the child must get the measles, 43 mothers said they wanted to get the illness over with, and 29 mothers said that they could not practically separate them.
D. Maternal Health
Over half the women in this sample said that they got married before they were 18 years old. Only 22% were older than 20 when they got married, and only 4% were older than 25 years old. 27% of respondents mentioned that their last child delivery was attended by a doctor. Only 16% of women surveyed said that they eat differently while they were pregnant, and, when probed, 70% of the total sample did not think that pregnant women need to eat differently.
E. Diarrhea And Dehydration
Diarrheal morbidity average about 43% of the 900 women surveyed. Of all respondents, 98% have heard of Oral Rehydration Solution (ORS), and 85% of them heard of it from television. Fifty-four percent of all Egyptian mothers interviewed in this survey have used ORS, but the percentage would be much greater if we consider only mothers whose children have had diarrhea.
Interestingly, when asked about causes of diarrhea, a very high percentage of women surveyed mentioned “cold” even though it was not one of the causes given in the Media campaign which has been underway for almost two years when the survey was conducted, which suggests the stubbornness of some public beliefs and the need to sustain public education programs over a relatively long period of time.
On the other hand, women have also learned specific preventive measures from the public campaign of the Oral Rehydration Therapy (ORT) Project. Thus, when asked what mothers should do to prevent diarrhea, most mothers mentioned “keeping the food clean,” “washing hands”, and also added, “protecting the child from catching cold!”
Women who did not use ORS were asked to state the reasons they had for not giving it to their children. Over 95% of those who did not give ORS said the reason was that diarrhea was light or that the child did not get dehydrated. A small number of mothers (5%) mentioned that the doctor did not prescribe it.
F. Subjects Which Mothers Want Television To Inform Them On
Mothers were asked if they wanted to get information on other health issues in the same way they got information on ORT. Of the 900 mothers surveyed, 85% answered the question positively. The percentages of issues which women mentioned that they needed more information on in new TV spots are listed below:
| Issue | Percent |
| Child care | 35% |
| How to treat diseases | 14% |
| General health care | 8% |
| Contraceptives and how to use them | 7% |
| Appropriate foods for infants | 7% |
| Maternal and child care | 7% |
| Hygiene | 6% |
| Pregnancy problems and care | 5% |
| Immunization schedules | 2% |
| Mentioned a variety of other issues | 10% |
G. Acute Respiratory Infections
Almost 81% of the total sample said that they heard of bronchitis. The symptoms most recognized by respondents are: cough, vomiting, fever, diarrhea, stomach ache, and wheezing. Over 95% of mothers said they took their children to see a doctor when they got bronchitis and only 5% gave medicine or other remedies before consulting a doctor.
To protect their children from respiratory infection, mothers mentioned specific actions such as keeping the child away from air drafts, keeping the child warm, and keeping the child clean. Over 10% of those familiar with bronchitis did not know how to protect their children from it. This, of course, is in addition to 19% who did not know what bronchitis was.
Mothers were asked whether or not their children caught cold during the two weeks preceding the interview. (Note that the study was conducted in the summer – from July through September- where infections are normally lower than winter time infections.) One out of four mothers said that at least one of her children had a cold. Two-thirds of the children with cold were seen by doctors, according to mothers’ responses.
H. Family Planning And Child Spacing
Respondents were asked to spontaneously name up to six contraceptive methods that women could use to space child bearing or prevent pregnancy. The following are the methods mentioned and the percentage of respondents which mentioning each of them:
| Contraceptive Method | Percent Knowledge |
| The Oral pill | 82 |
| I.U.D. | 76 |
| Injections | 43 |
| Spermicides | 18 |
| Condoms | 9 |
| Foaming Tablets | 7 |
| Sterilization | 2.6 |
| Diaphragm | 1.7 |
| Safe period | 0.3 |
We also asked these women about their source of contraceptive information. The following lists the sources and the percents of respondents citing each of them:
| Source of Information | Percent |
| Television | 78 |
| Other women | 12 |
| Health units | 11 |
| Radio | 8 |
| Other | 6 |
I. Home Hygiene And Space Allocation
Twenty percent of the women surveyed lived in one – roomed residences and 25% lived in two rooms. Another 25% lived in three rooms and 30% of the sample lived in residences containing four or more rooms. In terms of space allocation, 89% of the sample had rooms that were dedicated only to sleeping, 11% had rooms that were dedicated only to receiving guests, 10% had rooms that were dedicated only to living and only 1.6% had rooms that were specifically dedicated to dining.
Overall household hygiene in the homes of respondents was rated by middle class interviewers as follows:
| Good | 31% |
| Average | 41% |
| Poor | 28% |
Interviewers also observed whether the households they visited had bathrooms with soap and water. The results were as follows: 55% had bathrooms with soap and water, 39% had bathrooms which did not have either soap or water, and 6% did not have bathrooms. Furthermore, interviewers observed whether a towel was in or near the bathroom: 25% of the bathrooms had clean towels, 5% of the bathrooms had dirty towels, and 70% of the bathrooms had no towels.
J. Food Preparation And Hygiene
One-half of the women sampled said that they cooked in their kitchens and the other half cooked in rooms used for more than one purpose. Forty percent used a kitchen table to prepare their vegetables, while 12% used the low-round table called “Tablya” and 43% used the floor. The remaining 5% used other places.
Water
Sources of drinking water in the homes visited are followed:
| Water Source | Percent of Respondents |
| Piped Water | 57 |
| Hand Pumps | 22 |
| Public Taps | 11 |
| Tap in building or at Neighbor’s | 6.5 |
| Other | 3.5 |
Sewage
Types of sewage system in respondents’ homes:
| Sewage System | Percent of Respondents |
| Sewage well | 42 |
| Connected to Public Sewage System | 36 |
| Cesspools | 9 |
| Other means | 8 |
| Do not know | 5 |
Finally, the following household items were surveyed and their presence was identified as follows:
| Household Item | Percent Of Respondents |
| Electricity | 94 |
| Total Television | 91 |
| Black & white TV | 65 |
| Color TV | 26 |
| Radio | 82 |
| Washing machine | 68 |
| Tape Recorder | 66 |
| Fan | 51 |
| Stove | 49 |
| Refrigerator | 47 |
| VCR | 4 |
The Health Experts’ Survey
Doctors’ Perspectives on Egypt’s Health Problems
By: Farag Elkamel, December, 1985
(This study was conducted as part of the Sehettak Biddonia project, sponsored by the Ford Foundation, UNICEF, and the Johns Hopkins University)[1]
STUDY OBJECTIVES
This study has two main objectives: 1) to identify Egypt’s most important national health problems from the Egypt’s top doctors’ point of view; and 2) to identify the best methods through which mass media might deliver relevant health information to the public, also from the doctors’ point of view.
METHODOLOGY
One hundred top health professionals from several universities, the Ministry of Health (MOH), and other projects were selected to participate in this survey (see list of respondents). Participants were chosen on the basis of lists and suggestions acquired from university officials and the MOH. Each respondent was asked to complete a questionnaire of seventeen questions regarding pressing health problems and methods of disseminating information about them. The study was conducted by the Center for Development Communication between July and November 1985.
Seventy-six of the 100 respondents were connected to universities, 15 with the MOH, eight with health projects, and 12 with other institutions. (Some were connected with more than one category of the above.)
Respondents represented a variety of professional experience. Thirty-six respondents were professors, 10 assistant professors, 30 lecturers and assistant lecturers, 15 MOH administrators, 8 project officials and 1 that could not be classified in any of these categories.
Most respondents (54) specialized in pediatrics. Of the rest, 17 specialized in public health, 5 in pharmaceutics and 24 in other assorted fields.
STUDY DIFFICULTIES
Certain problems were encountered during field work:
- Many selected participants from the university were on vacation during summer field work, which delayed their responses.
- Some selected respondents did not return surveys promptly for other reasons.
- The application procedure for the necessary official permits for the project is lengthy. First, the Central Agency for Public Mobilization and Statistics (CAPMAS) required three weeks to process the application. Second, the Ministry of Health and its security needed at least another week to issue the subsequent permit.
- Open-ended survey questions needed complex and lengthy analyses requiring extra time, though the information gathered was worthwhile.
FINDINGS
1. Important National Health Problems
IN YOUR OPINION, WHAT DO YOU THINK ARE THE TEN MOST IMPORTANT HEALTH PROBLEMS IN EGYPT? COULD YOU ARRANGE THEM IN ORDER OF IMPORTANCE?
The first question concerns the ten most important health problems in Egypt. Respondents were asked to arrange these problems in order of importance. While all of the participants answered the question, not all gave ten answers.
Respondents indicated the most important health problem as being malnutrition, followed by diarrheal and gastroenteritis diseases, endemic parasitic diseases, infectious diseases, chest & respiratory diseases. They also mentioned pollution and bad sanitation as causes for many of these health problems. The category “infectious” encompasses general problems, mainly focusing on those requiring immunization. Tuberculosis, polio and measles, which also require vaccinations, are listed as separate categories being mentioned specifically by respondents.
2. Ideal Methods for Disseminating Information
WHAT DO YOU THINK IS THE BEST METHOD(S) TO DISSEMINATE INFORMATION TO THE PUBLIC ABOUT THE PROBLEMS YOU MENTIONED?
WHAT DO YOU THINK IS THE BEST METHOD(S) TO DISSEMINATE INFORMATION TO THE HEALTH PROFESSIONALS TO KEEP THEM INFORMED OF UP-TO-DATE DEVELOPMENTS?
In order to best disseminate information both to the public and to health professionals of up-to-date developments, respondents were asked to chart the value of various channels, including personal counseling, lectures and talks, radio, television, press, films, pamphlets, booklets, posters, community organizations and other suggestions.
- Reaching the Public. To reach the public, most respondents (91%) chose television as selected method, followed 66% choosing by radio, 50% personal counseling and 40% community organizations. Films were less desirable, chosen by 29%, as were lectures (20%), press and posters (18%). Of the remaining choices, 8% chose booklets and 4% gave other answers. Only 1% failed to answer the question.
- Reaching the Health Professionals. To reach the health professionals, the highest percentage of respondents, 67%, chose lectures and talks. Pamphlets seemed useful to almost half of the group, or 43%, as did booklets, which were chosen by 41%. 28% selected personal counseling and 15% press and films. Each of the other categories received less than 12%. 5% of the respondents did not answer this question.
3. Formats for Health Information
WHICH FORMATS WOULD YOU PREFER HEALTH INFORMATION TO BE PROVIDED TO THE PUBLIC IN? PLEASE ARRANGE IN ORDER OF PREFERENCE.
Respondents were asked to arrange the following format choices in order of preference. These formats represent preferred methods of providing health information to the public. Only 1 % of the respondents did not answer the question, but several checked boxes without ranking their choices.
As the number one choice, out of 86 answers 20 of them said interviews with mothers, 19 said drama, and the same number said songs. Interviews with health professionals and commercials were chosen by 13 each and prize competition and others by 1 each. As the second preference, out of 81 answers, 22 said interviews with health professionals; 18 said interviews with mothers; 17 said drama; 12 said commercials; 7 said songs; 3 said prize competitions. Combining all of the rankings, 75% chose drama and interviews with mothers and health professionals as a preferred format, closely followed by commercials receiving 72% of the total response, songs 65% and prize competitions 48%. Thus it appears that generally, interviews with mothers and health officials and drama are the popularly recommended formats by the respondents.
4. Key Interventions to Reduce Child Morbidity and Mortality
THE FOLLOWING MEASURES WERE IDENTIFIED AS KEY INTERVENTIONS TO REDUCE CHILD MORBIDITY AND MORTALITY IN EGYPT. FOR EACH INTERVENTION, PLEASE SPECIFY WHETHER YOU THINK IT WILL BE VERY EFFECTIVE, SOMEWHAT EFFECTIVE, OR NOT EFFECTIVE.
THEN, FOR EACH OF THESE INTERVENTIONS, PLEASE SPECIFY WHAT THE PUBLIC SHOULD KNOW AND/OR DO.
The next question identifies key interventions to reducing child morbidity and mortality in Egypt: Oral Rehydration Therapy, Immunizations, Breast Feeding, Water Supply and Sanitation, Personal and Domestic Hygiene, Weaning Practices, Food Hygiene and Protecting Pregnant Mothers against Tetanus. Respondents were also asked about the effectiveness of intervention and what the public should know and do.
1. Oral Rehydration Therapy.
For the use of oral rehydration, 74 responded that it is very effective, 21 somewhat effective, and 1 person said that it was not effective. 4 did not respond. 68 of the respondents gave explanations. Most of these explanations (23) said ORT was effective because it was able to decrease diarrhea and dehydration. 17 others said that it was easy to use, 16 people mentioned that it was easy to prepare, 13 liked its low cost, 10 that it was easy to obtain, 9 that it was useful in severe cases and 3 that it was safe.
What the Public Should Know and Do
Respondents were also asked to identify what the public should know and do. Most (37) said that the public should know exactly how to prepare and use the solution, while 10 respondents noted that the public should know when to administer the therapy, its effectiveness and to be sure to consult a doctor or hospital. Other suggestions include warning mothers to continue breast feeding, telling parents where to obtain the fluid and when it’s useful, and of complications and benefits.
2. Immunization: the Triple Vaccine
For the triple vaccine immunization, 41 persons found this intervention to be very effective. 9 respondents explained that its efficiency was effective while others noted that it is a good prevention of serious diseases, that there is currently a low incidence of these diseases, and that the routine practice is familiar to all.
What the Public Should Know and Do?
On the other hand, respondents identified what they thought the public should know and do regarding this vaccine. 7 people said hazards of the disease should be known. 5 others said timing of vaccinations should be stressed, as well as its importance. The public should also know the importance of spacing between doses, complications after vaccination, where to get vaccination, and about contraindication.
3. Vaccination for Measles
Out of the 24 respondents who believed this vaccination to be very effective, half gave some explanations. 5 respondents thought this particular immunization to be able to prevent scars, others noted the widespread waves of the disease, and that there are high cases fatality. One person mentioned that two doses are needed, as are booster shots.
What the Public Should Know and Do
When asked what the public should know and do, respondents believed that people should be told about booster doses, how the vaccination prevents diseases, about timing, and the proper site of injection to avoid nerve paralysis.
4. Vaccination against Polio
Of the 47 who believed this vaccination to be very effective, 10 explained that it was effective in abolishing or decreasing the incidence of polio, while 2 said that it was successful in that it was easy to take.
What Public Should Know and Do
When asked what the public should know and do, the respondents suggested that people should know of polio’s complications, about timing, its method of administration and about booster doses.
5. Immunization in General
Among the respondents who answered that immunization as a whole was effective, 24 responded that it was very effective. If given as a prophylactic, immunization can reduce morbidity. Compulsory programs were recommended, put into effect with mass media campaigns. Also, due to the aggregation of the population, health units, primary health care and private clinics could be used to help the mass media spread information.
What Public Should Know and Do for Vaccinations
In reference to what the public should know and do for the three vaccinations together, 34 respondents replied that proper timing should be stressed. 17 said that the public should know of the value of the vaccination and its effectiveness. The dangers of disease and difficulty in treatment were mentioned by 13 others. Other recurrent answers were to inform where to obtain the vaccinations, possible precautions and side effects, and about the timing of booster doses and age to be administered. Some mentioned that the public needs more information, which may be served by mass media and personal contact.
6. Promotion of Breast Feeding
70 of the respondents believed the promotion of breast feeding to be very effective. 11 respondents reasoned that it was a cheap supply of nutrition, while 10 noted that it decreases diarrhea and gastroenteritis, which artificial milk can stimulate. 7 people remarked that it was easily available, clean, and contains antibodies which gain immunities for the child. Others noted the psychological benefits to mother and child, and its use in preventing malnutrition and most infectious diseases. It is also culturally acceptable, and a natural form of child spacing. Also, bottle feeding can be expensive. Even for working mothers, in rural and urban low socioeconomic brackets, breast feeding is well practiced and high biological value. There were also suggestions to introduce informative health units in clinics, television and radio and to form a health nucleus for the community.
What the Public Should Know and Do
In the next question, respondents were asked what the public should know and do. Most persons (48) emphasized that the public should know advantages to mother and baby and the disadvantages of artificial milk. Also, the public should know the role of breast feeding in prevention of infection and in increasing immunities to protect the child’s health. Also, perhaps the public should be informed of proper timing and how to prepare for it.
7. Adequate Water Supply and Sanitation
Of all the respondents, 65 said this would be very effective. 38 found that as a prophylactic, it would prevent or reduce water and food borne infections, as well as diarrheal diseases. As a hygienic environment, a sanitary water supply would promote general health if readily available.
What the Public Should Know and Do
When asked what the public should know and do, most stressed its importance in preventing diseases and its advantages. Also, the public should know how to use and obtain sanitary water. A few mentioned the need to work closely with the government.
8. Promotion of Personal and Domestic Hygiene
48 of the respondents believed this to be very effective. Of these, 26 said that as a prophylactic against microbes and infectious diseases it would be very useful. Also, personal hygiene would be good for general health practices.
What the Public Should Know and Do
In response to what the public should know and do, 18 noted the advantages in prevention and eradication of infectious diseases as prominent. 26 stressed the public’s need to know how, and 20 others why. A few respondents mentioned that a religious approach might be effective.
9. Improved Weaning Practices
Out of all 100 respondents, 40 believed improving weaning practices to be very effective. 25 of these 40 said that it would improve health and prevent serious nutritional disorders, diarrhea and gastroenteritis. Others mentioned that it decreases psychological problems, and provides a nutritional supplement to breast milk. Also, MOH centers should improve facilities.
What the Public Should Know and Do
When asked what the public should know and do in reference to weaning practices, 23 emphasized how, or the ideal weaning details of food for each month, and 20 others stressed what kind of food to give the baby. 16 mentioned timing, and 26 others wanted the advantages of good weaning practices to be known. Others noted the need to provide well-trained, adequate facilities and education.
10. Improved Food Hygiene
44 of the respondents replied that improving food hygiene would be very effective. 29 felt that it would prevent diseases, such as diarrhea, gastroenteritis, and food poisoning, as well as nutrition disorders. 2 people noted that communities also need sanitary water and general sanitary conditions, in addition to education on community and personal levels.
What the Public Should Know and Do
The respondents were then asked what the public should know and do about food hygiene. Most people stressed how, or what sanitary means were available for preparing and keeping food. Others stressed its importance, in preventing diseases transmitted through flies and other insects. Others mentioned the responsibility of government to inspect milk shops, meat shops and restaurants.
11. Immunization of Pregnant Mothers against Tetanus
42 of the respondents believed that immunizing pregnant mothers against tetanus would be very effective. 22 said that it prevents tetanus which is common and serious, and neonatal tetanus, since many babies are delivered by midwives in unsanitary conditions. Others noted that it was easily organized and implemented, and thoroughly advantageous.
What the Public Should Know and Do
Numerous and varied answers were given to the question of what the public should know and do. 24 stressed the need to inform the public of its advantages and importance, while 19 wanted to emphasize proper timing. Others noted that the public should know of possible dangers of tetanus on physical and mental development of children and the importance of personal hygiene and sterile conditions during birth. Also, a program should tell the public how and where to obtain the vaccine, and make sure facilities are indeed available.
5. Other Measures to Reduce Mortality and Morbidity
WHAT OTHER MEASURES DO YOU THINK COULD BE EFFECTIVE IN REDUCING CHILD MORBIDITY AND MORTALITY IN EGYPT?
The following question asks respondents what other measures might be effective in reducing child mortality and morbidity in Egypt. The subsequent paragraphs summarize the responses of the 79 who answered this question.
- Family planning and Birth spacing. 16 of the respondents maintained that family planning and spacing was important to children’s’ health.
- Education. 35 mentioned education as an effective measure, while some specified health education and others education to mothers. Some believed illiteracy to be the factor needing to be eliminated. Some respondents stressed the need to introduce health topics in schools for children, others the need to educate in rural areas, perhaps using students during summer holidays. Many mentioned the role of television in health education. Finally, some responded that medical and paramedical professionals need to continually be educated.
- Health Services. 22 of the respondents answered that improving health services would be an effective measure in reducing child mortality and morbidity in Egypt. Some places that were specified include maternal child health facilities, general street clinics, hospitals, health delivery systems, places outside big cities, institutes for handicapped children, specialized centers for children and pediatric hospitals. Specific practices to be watched carefully and improved include diagnosing diseased children, caring for newborn and genetically determined diseases, C.N.S. injection, overuse of instrumentation during birth resulting in brain damage, obstetric care, neonatal services, and antenatal care. Information is needed about the effect of drugs and nutritional problems, and more medical care is needed.
- Economic and Social Development. 16 of the respondents said that raising the socioeconomic level of people and improving jobs and wages for workers would be an effective measure in improving children’s’ health.
- Others. Other varied responses include proper psychological care for children; community participation; prevent leading causes of morbidity and mortality; use mass communication; improve health awareness; recognize early manifestation of common problems; use day care centers; reduce traffic accidents; fight bilharzias; leave mothers free to handle children during first 3 years; hazards of drugs, especially stimulants in secondary schools and addictions. Some respondents repeated measures all ready discussed within the questionnaire. These include sanitary environment (10), immunizations and vaccinations (7), nutrition (7), hygienic conditions, ORT and breast feeding (3).
6. Current ORT Mass Media Campaign
PLEASE COMMENT ON WHETHER THE FOLLOWING ASPECTS OF THE CURRENT ORT MASS MEDIA CAMPAIGN ARE GOOD OR NOT GOOD AND WHY: CONTENT, FORMAT, DURATION AND TIME OF BROADCAST.
To help decide whether or not to adopt the same technique for other health problems, respondents are asked whether the following aspects: content, format, duration and time of broadcast, of the ORT mass media campaign are good or not, and why.
- Content. Most respondents (76) considered the content to be a favorable aspect. Twenty-two explained that the content was good because it was simple and easy for the public to understand. Others replied that the content was well studied and covered important information, while seven offered no explanation. Most of the explanations given by the 13 who said that the content was not good focused on the incompleteness of the information offered, which may lead to misunderstanding. Some feared that mothers would stop seeking medical advice, misuse the treatment and assume it’s the only and proper solution for each case.
- Format. Of all the respondents, 78 said the format was good. Sixteen respondents liked the format because it was attractive and interesting, two noting the popularity of the actress. Twelve explained that the short, simple, and concise format style was good, and five expressed that television was an excellent medium for reaching the target audience. The 10 respondents not liking the format explained that the songs were not serious, the appeal was not scientific, and perhaps required more explanation.
- Duration. Of the 100 persons surveyed, 73 liked the length of the messages. Twenty-four respondents explained that the length of commercials were good not being time-consuming, requiring much attention and able to be repeated. Four explained that the frequency was appropriate and they believed the conciseness kept the message interesting. Three people thought the duration of the message to be too short, one too long; one believed the message to be too frequent, another two, not frequent enough. Thirteen people offered no explanations at all for their opinions.
- Time of Broadcast. Seventy-nine respondents liked the time of the broadcast. Eighteen respondents explained that the time of broadcast was good in that the families were usually gathered at that time to watch television. Five others noted the good position in the broadcasting schedule, being before popular dramas. Eighteen believed it to be good but offered no explanation. Four of the eight respondents who believed the time to be not good offered some of the following explanations: other evening times might be better; could also be before comedies, films and football matches.
7. Child Immunization Coverage
WHAT DO YOU THINK ARE THE REASONS UNDERLYING THE OBSERVED LOW CHILD IMMUNIZATION COVERAGE WITH THE TRIPLE VACCINE AND MEASLES VACCINE?
Recently, child immunization coverage with triple and measles vaccines has been observed to be low. Respondents were asked what they thought to be the underlying reasons for this. 22 felt that ignorance, negligence, carelessness of mother or parents were the main reasons, while 16 others found faults that there were not enough publicity campaigns or general education. Again, bad storage techniques, especially in villages were mentioned by 9 persons. Others noted the high level of poverty, illiteracy and unacceptability in rural remote areas. Also, the vaccine was unavailable in many markets.
- Triple Vaccine. In reference to the triple vaccine, again ignorance of mother or parents was given as the cause for low coverage by 26 persons. 12 people said that repeated doses are needed, which should be added to currently deficient health education and mass media campaigns. The bad behavior and attitudes of health personnel were also a problem. A few noted the expense of vaccine and poverty of people may contribute to this low coverage.
- Measles Vaccine. As to the measles vaccine, again culture and tradition (the disease is considered a gift from god and not harmful) was mentioned as the root cause for low use by 12 persons. 9 others pointed to a failure of the vaccine itself. Again, a lack of health education, facilities expense and availability were mentioned as problems.
8. The Polio Campaign
PLEASE COMMENT ON WHETHER EACH OF THE FOLLOWING ASPECTS OF THE PAST POLIO CAMPAIGN IS GOOD OR NOT, AND WHY: CONTENT, FORMAT, DURATION AND TIME OF BROADCAST.
In the following question, people were asked to comment on the content, format, duration and time of broadcast of the polio campaign.
- Content. 68 respondents believed the content to be good. Most of the respondents explained that the content was well-done (8) and effective (7). Also, they said that the message was simple and easily understood (5) and polio in fact was decreasing (2). Others believed that the content could be livelier and include more details. 8 people did not like the content, explaining that it emphasizes paralytic polio, is not attractive, not completely scientific and there is no mention that vaccinations should not take place on street roads, but in health centers.
- Format. 66 people thought the format was a good one. Their reasons include that the format is well-done (5), easily understood (3), short (2), attractive (3) and accepted (2). One person thought it should be more often, another not enough. 11 respondents replied that the format was not good for these reasons: more stress needed on morbidity and mortality; use songs and films; too short (2); more drama and interviews with mothers and doctors; too authoritative.
- Duration. 58 of the respondents were pleased with the duration. Most believed the duration to be suitable (8), while some specified the short length as being good in not consuming much time (4). Others remarked that it was effective (3) and that the evening time (1) and frequencies (1) were working well. 17 people did not like the duration. Of these, 7 respondents though the duration to be too short, and the other 2, too long.
- Time of Broadcast. 62 respondents liked the time of broadcast. Most responded that it was suitable (8), others that the evening time was good (4), summer time preferable (1) and that positioning should be before drama, films and sports matches. 10 people gave no explanation but believed it to be good, and two people said it was not good without explanation. Of the 8 that explained it to be not good, some believed it to be not suitable for all women (2) and not to be shown at the right time (1).
9. Strengths of Existing Health Programs
WHAT ARE THE STRENGTHES OF THE EXISTING HEALTH PROGRAMMES ON RADIO AND TV? PLEASE COMMENT ON CONTENT, FORMAT, DURATION AND TIME OF BROADCAST.
The next question asks respondents to comment on the strengths of existing health programs on radio and television. 40 people answered this question.
- Content. 29 respondents commented upon the content of the programs. 14 of the respondents thought the content to be good; 4 said it to be clear and easily understood and 4 others comprehensive but 3 others found that the content was a mixture of good and not good.
- Format. 32 respondents discussed the strengths of the formats, while 8 people did not answer. 15 liked the formats, and 5 thought it easily understood, 4 said fair, and 1 effective. Two people did think the format could be revised.
- Consistency. 22 people responded to the question of consistency. 12 People specifically said that they liked the consistency, but 4 thought it should be strengthened. Others recommended that it be simple, effective and attractive, while one responded only for the ORT campaign. 18 people did not answer.
- Language. As to the language, 32 people provided answers, while 8 did not. 22 preferred use of native, slang language, while 4 others thought Arabic should be used to target educated persons. 19 the 28 respondents thought scheduling was well-done. Others recommended evening and afternoon hours, weekly times, and before news and movies. 12 people did not answer this section.
10. Weaknesses of Existing Health Programs
WHAT ARE THE EXISTING HEALTH PROGRAMMES ON RADIO AND TV? PLEASE COMMENT ON CONTENT, FORMAT, CONSISTENCY, LANGUAGE AND SCHEDULING.
Respondents were then asked to comment on the weaknesses of existing health programs on radio and television. 40 people did not answer at all.
- Content. 23 of the 37 people answering found fault with the content, as being not detailed enough or providing wrong information. 7 others said the content was not well understood or interesting and 2 said it was ineffective. Only 2 thought it to be adequate. 7 did not answer this question.
- Format. 27 responded to the format section. The format is also found by 8 to be lacking in adequate information, 7 said it was not well organized, 6 that it was unattractive, 4 not easily understood and 2 replied that it varied. 17 people did not answer this section.
- Consistency. 21 people responded to the consistency. 8 believed not enough was said about various problems, 4 others that it was too complex, 3 that it was not attractive and 2 that generally not very good). 23 people chose not to answer this question.
- Language. 20 people did not respond as to their opinions on language, but of the 24 who did 18 preferred simple, native languages that would be easily understood. Only a few offered differing responses: language should be more scientific (2); less vulgar (1); in English (1).
- Scheduling. 9 of the 16 respondents answering the next section believed the scheduling to be disorganized, 5 said it was not working well and another 5 said not frequent enough.
- All Aspects. When asked to respond as to those aspects all together, 16 People gave the following answers: too complex, not simple and direct enough (4); unorganized (4); boring (2); needs more promotion (1); no weaknesses at all (2).
11. Guidelines for Health Planners
WHAT DO YOU THINK ARE THE MOST IMPORTANT 5 PRECAUTIONS PLANNERS OF HEALTH EDUCATION PROGRAMMES SHOULD BE AWARE OF?
In the last question, respondents are asked what five most important precautions planners of health education programs could be aware of (12 % did not answer this question).
- Baseline Study. In reference to a primary study, several varied answers include: should know culture, tradition and habits of Egyptians (26); know health needs of population (14); the age group of target population and how to reach them (11); their level of education (13); their socio-economic level (4); literacy and intelligence level (8); religious beliefs and how to deal with them (6); and more about the population, such as how they live, number of children in each family, where mothers live, free time of mothers, and more about parents in general.
- Health Programs. Planners of health programs should also be careful to make campaigns attractive (4), not too scientific or frightening (4), valid, correct and clear (9), thorough (5), not too frequent (2) but frequent enough (7), reasonable, suitable time of broadcasting to audience and prominence of disease (10), to consult with health professionals and experts, to avoid abuse or overdose of knowledge (2), utilize message harmony with programs, show public dangers of problem (2), and choose the right person for this message (some prefer popular personalities and others desire prestigious health personnel with high education.
- Language. 19 respondents mentioned language as one of the important precautions after knowing the target population. The language chosen should be easily understood, simple, and common.
- Health Education. In reference to health education, respondents desired more health education facilities; more health education to mothers (3), medical students and doctors; health education in nursery and schools; use of audio visual means, films and television (2); importance of basic scientific message; right method to reach professionals; maternal education in nutrition, weaning and hygiene of infants.
- Other Precautions. Other precautions mentioned include being aware or availability and feasibility, to plan for an independent evaluation, to note the existing gap between the community and government, to not forget non-traditional approaches of informing the public and to study problems in the field before advising the public.
[1] It should be noted that a parallel study was conducted with a sample of the general public. It should be interesting to compare the findings of the two studies, which are published in this site.
Participants in the health experts’ survey, by alphabetical order:
- Dr Abdel Rahman Ahmady, Pediatrics, Al Azhar University
- Dr Abdel Moniem Youssef, School Health Administrator in H M , M O H
- Dr Ahmed Nagaty, SRHD Project
- Dr Ahmed Yehia Darwish, Abu El Rish Hospital, Cairo University
- Prof Ahmed Mohamed Abou Hassan, Pediatrics, Cairo University
- Dr Ahmed Saad El-Din El-Beleidy, Pediatrics, Cairo University
- Dr Ahmed Swedan, Pediatrics, Cairo University
- Dr Ahmed Hashem Abd el Aziz, Director General of Urban P H C , M O H
- Prof Ahmed Hanafi Mahmoud, Community Medicine, Cairo University
- Aisha El Marsafy, Pediatrics, Cairo University
- Prof Amal El-Beshlawy, Pediatrics, Cairo University
- Dr Amin Kamel Said, Head Clinical Nutrition Dept , Nutrition Institute
- Prof Amina Hendawy, Pediatrics and Neurology, Cairo University
- Prof Amira Salem, Pediatrics, Cairo University
- Prof Anissa M El Hefny, Pediatrics and Clinical Immunology, Cairo University
- Prof Awatef El Mazni, Pediatrics, Cairo University
- Prof Baheia Mostafa, Pediatrics and Nephrology, Cairo University
- Professor Bayoumi El Sibaie, Pediatrics, Cairo University
- Prof Bothina M El Naggar, Pediatrics, Al Azhar University
- Mr Effat Ramadan, N P C and Executive Director of F O F
- Ms Effat Ibrahim Kamel, Director of the General Nursing Department, M O H
- Dr Entissar M El Sabbar, General Director of M O H
- Dr F A Saleh, Epidemiologist, M O H
- Prof Fadia Mohamed Ali, Pediatrics, Cairo University
- Prof Farida Faried, Pediatrics, Ain Shams University
- Dr Farouk Shaheen, Nutrition Institute
- Dr Fawzan Shaltout, Pediatrics, Cairo University
- Prof Fawzi Gadalla, Community Medicine, Al Azhar University
- Prof Fouad El Behairy, Pediatrics, Al Azhar University
- Dr Gamal El Din Abdel Aziz, NCDDP
- Prof Gilane Abd El Hamid Osman, Pediatrics, Ain Shams University
- Dr Hala Fouad, Pediatrics, Cairo University
- Dr Hassan Belal, Head of Communication Department, M O H
- Dr Hamida Mohamed El Gohary, Faculty of Pharmacy, Cairo University
- Professor Hekmat El Ghadban, Pediatrics, Cairo University
- Dr Hoda Ibrahim Fahim, Public Health, Ain Shams University
- Dr Hoda Seoud, Pediatrics, Al Azhar University
- Dr Hosni Mohamed Mahrous, Marketing Coordinator, NCDDP
- Prof Hussein El Nahal, Bilharzias Institute
- Dr Ibrahim Fouad, Public Health, Cairo University
- Dr Ibrahim Farrag, Director General of Fever Hospital Dept , M O H
- Dr Ibrahim S Hegazy, Public Health, Cairo University
- Dr Iman Abd el Salam Seoud, Pediatrics, Cairo University
- Dr Jerry Russell, Public Health, NCDDP
- Dr Kadry Wishahy, Pediatrics, Cairo University
- Prof Karima El Zawahri, Pediatrics, Cairo University
- Prof Laila Mahmoud Kamel, Public Health, Cairo University
- Dr Lamis Ragab, Pediatrics, Cairo University
- Dr Madiha Said Mohamed, Public Health, Cairo University
- Dr Magda Mohamed Fathy, Faculty of Pharmacy, Cairo University
- Prof Magdy El Barbari, Pediatrics, Cairo University
- Dr Maha Moustafa Kamel Mourad, Pediatrics, Cairo University
- Prof Maher Mahran, Secretary General of NPC and OBGYN at Ain Shams University
- Dr Mahi Mahmoud Fahim, Public Health, Ain Shams University
- Dr Mahmoud Radwan Mohamed, Public Health, Ain Shams University
- Prof Mahmoud Essawi, Pediatrics, Ain Shams University
- Prof Mahmoud Taher El Mougi, Pediatrics, Al Azhar University
- Prof Mamdouh Kamel Gabr, Chairman of Pediatrics, Cairo University
- Dr Mansour M Al Okka, National Control of Diarrheal Disease Project
- Prof Mervat El Rafie, Public Health, Cairo University
- Dr Mogedda Mohammed El Ayoubi, Pediatrics, Cairo University
- Dr Mohamed Naur Abd el Wahab, General Director of M C H , M O H
- Dr Mohamed Said Ibrahim El Sayed, Pediatrics, Cairo University
- Dr Mohamed Atteya, General Director of Health Education and Information
- Prof Mohamed Khayyal, Faculty of Pharmacy, Cairo University
- Prof Mohamed Fouad El Badrawy, Pediatrics, Ain Shams University
- Dr Mohamed El Mosalamy, Public Health, Al Azhar University
- Dr Mohamed Amr Hussein, Nutrition Institute
- Dr Mohamed Galal Mahmoud, Department of Curative Medicine, M O H
- Dr Mohamed Fahmy Ameen, Al Azhar University
- Dr Mohsen Gadallah, Public Health, Ain Shams University
- Dr Mona Hassan El Tagy, Pediatrics, Cairo University
- Dr Mona Soliman Mohamed, Public Health, Cairo University
- Dr Mona Zahran, Bilharzias Institute
- Dr Mostafa Hamami, Vice Minister of M O H for Primary Health Care and Family Health
- Dr Nadia Mostafa, Pediatrics, Cairo University
- Dr Nahed Amer, Pediatrics, Cairo University
- Dr Nahed Fahmy Helal, Mounira Children’s Hospital
- Dr Naira El Akkad, Pediatrics, Al Azhar University
- Dr Narges Albert Labeeb, Public Health, Cairo University
- Dr Norman Kaddah, Pediatrics, Cairo University
- Dr Osman Galal, Director of the Nutrition Institute
- Prof Rabah Shawky, Pediatrics, Ain Shams University
- Dr Rabha El Shenawy, El Mounira Pediatric Hospital
- Prof Ramzi El Baroudy, Pediatrics, Cairo University
- Prof Saadia Abdel Fattah, Pediatrics, Ain Shams University
- Dr Said Madkour, MCH Specialist, M O H
- Prof Salah Kamel Nassar, Pediatrics, Cairo University
- Dr Salah Madkour, General Director for Communicable Disease Control Dept, M O H
- Dr Salwa Abdel Aziz, Public Health, Cairo University
- Prof Susan Amin El Sokkary, Pediatrics, Ain Shams University
- Dr Samia Nour, Pediatrics, Cairo University
- Prof Samiha Samuel Wissa Doss, Pediatrics, Cairo University
- Dr Sanaa Ahmed Aly, Pediatrics, Cairo University
- Dr Sowsan Abd El Hady Hassan, Pediatrics, Cairo University
- Prof Sayed Hilal, Dean of Faculty of Pharmacy, Cairo University
- Prof Shafika Saleh Nasser, Community Medicine, Cairo University
- Prof Soad Ishaac Wahba, Pediatrics, Cairo University
- Prof Taha S El Alfy, Faculty of Pharmacy, Cairo University
- Dr Wafaa Moussa, The Nutrition Institute
Media and Health Education Conference, Etap Hotel, Ismailia, Egypt
January 10 and 11, 1986


Summary of Conference Recommendations
Participants of the “Mass Media and Health Education Conference” that was held in Ismailia on January 10 and 11, 1986, reviewed and discussed the “Sehettak Biddonia Project.” They examined the Project’s components and focused on baseline studies[i] which were conducted by the Center for Development Communication (CDC). Participants held extensive discussions and formulated specific remarks about and recommendations for the project.
Participants strongly support the Sehettak Biddonia Project’s scientific and systematic approach of using communications and social marketing techniques to improve the public’s health standards and quality of life through this health education program. They also assert that the Project significantly contributes to national development as it addresses a real need for public information on health issues. The participants emphasize that the project would lead to improved health whcich benefits every citizen whether (s)he be a woman, man, or child.
This is a summary of the recommendations for the Sehettak Biddonia Project, as outlined by the participants in this “Media and Health Education Conference.” organized by CDC and the donors of the project.
A. Pool of Health Issues and Problems
The conference participants pointed out a valuable source of health issues for the Sehettak Biddonia Program to focus on which is the extensive “Health Profile Survey”, conducted by the Ministry of Health. Other sources are the results of the 100 health experts and 900 mothers surveyed by CDC as well as the Mass Media and Health Education Conference itself.
B. Criteria for Establishing Health Priorities
The workshop participants maintain that criteria for establishing health priorities include the following:
- Prevalence
- Severity (causing death / disability)
- Community concern
- Social impact
- Can be affected by information
- Preventability (health problems that can be prevented by behavioral change)
- Existing Infrastructure (issues which have an existing health services infrastructure takes higher priority over those that require creating new services.)
Health problems and issues should be given scores on each of the above criterion and prioritized according to the order of those scores. The issue with the highest score takes highest priority.
C. Scoring
Participants recommend that CDC evaluate and prioritize health problems and issues in the way described above. They further recommend that the draft be evaluated by judges comprised of experts identified by CDC and the Ismailia Workshop participants.
D. Health Issues of Highest Priority
Participants ranked health issues according to the priority in which issues should be covered by the Sehettak Biddonia Program. It was agreed that the following four issues take highest priority:
- Immunization: campaigns should aim to fortify the present immunization schedule and program
- Malnutrition of children and adults
- Personal hygiene
- Reproductive health
Additional priorities will be established through the process described in A, B, and C, above.
E. Supportive Infrastructure
Participants believe several factors , which are beyond the control of the project, can reinforce the “Sehettak Biddonia” project impact:
1. Continuing improvement of the health delivery system in these areas:
- Management
- Nursing
- Service quality
- Equipment
- Health professionals’ continuous in – service training
2. Communication messages should be synchronized with service availability.
F. The Socioeconomic Environment
The following socioeconomic factors positively or negatively affect the four health issues in `D’ above should be considered when designing messages:
- income
- economic constraints
- traditional modes of production
- beliefs
- level of health information already possessed
- status of women
- child labor exploitation
- level of formal education
- Interrelations between the four health issues
G. Target Audience
- Illiterates and low-income level groups will be especially targeted.
- Some messages will mainly address women
- Some messages will target men
- Some messages will be aimed at all family members
The detailed report also includes comments that
have been given throughout the conference and elaborated upon during group
discussions and presentations.
[i] The baseline studies reviewed by conference participants were: 1) “Highlights of the Health Experts Survey on Basic Health Issues in Egypt; and 2) “Highlights of Mothers’ Knowledge, Attitude, and Practice Survey on Basic Child Survival Communication Issues.”
List of People Invited to Attend the Conference According to Alphabetical Order of First Names:
- Dr. Ahmed Nagaty, Strengthening the Rural Delivery System, MOH
- Mr. Ahmed Bahaa el Din, Writer, Al Ahram Newspaper
- Dr. Ahmed Foad el Sherbini, Professor and Dean of Public Health Institute, Alexandria
- Dr. Ahmed Khasab, Professor of Pediatrics, Benha University
- Dr. Ali Agwa, Vice Dean, Faculty of Communications, Cairo University
- Ms. Amal Mikawy, Director of Channel One, Television
- Ms. Ann Crowly, Catholic Relief Services
- Mrs. Aziza Hussein, Cairo Family Planning Association
- Dr. Barbara Ibrahim, Ford Foundation
- Ms. Connie Collins, Child Diarrheal Disease Control, United States Agency for International Development
- Mr. Edward Lannert, Country Representative, UNICEF
- Mr. Effat Ramadan, National Population Council and Director of F.O.F.
- Mrs. Elham Fateem, F.O.F. Research Department Director
- Dr. Ez el Din Osman, Professor and Head of Gynecology and Director of Fertility Care
- Mr. Fahmy Omar, President of Egypt Radio
- Dr. Fahyma Mohamed Hassan, Menoufia University, Pediatrics
- Dr. Farouk Abou Zeid, Cairo University
- Dr. Farouk Shaheen, Nutrition Education Project
- Dr. Fawzy Gadallah, Prof. of Community Medicine, Al Azhar Univ.
- Dr. Reginald Gibson, Oral Rehydration Therapy
- Dr. Gihan Rashty, Vice Dean of Communications & Head of Radio Dept., Cairo Univ.
- Dr. Gilane Abd el Hamid Osman, Professor of Pediatrics, Ain Shams University
- Dr. Hassan Belal. Head of Communications, M.O.H.
- Mrs. Hind Khattab, American University in Cairo
- Dr. Hosein Amer, Head of Epidemic Control, M.O.H.
- Dr. Ibrahim el Kerdany, UNICEF
- Dr. Jerry Russell, John Snow, Inc./ NCDDP
- Dr. Judy Barslow,Ford Foundation
- Dr. Kamal Ismail, Security Department, M.O.H.
- Dr. Laftaya el Sabaa, Egypt Television
- Dr. Laila Mahmoud Kamel, Professor of Public Health, Cairo University
- Dr. Lee Travers, Ford Foundation
- Ms. Liz Taylor, National Population Council
- Dr. Maher Mahran, National Population Council
- Mr. Khashab Matheme, UNICEF
- Dr. Mahmoud Essawi, Professor of Pediatrics, Ain Shams University
- Dr. Mahmoud Taher el Mougi, Professor of Pediatrics, Al Azhar University
- Dr. Mahmoud Hafez, Professor of Pediatrics, Zagazig University
- Dr. Mamdouh Gabr, Director of Pediatrics, Abou Elrish Hospital, Cairo Univ.
- Dr. Mansour el Okka, Oral Rehydration Therapy
- Ms. Marlene Kanawati, Oxfam
- Dr. Martin Ochs, Chairperson, Mass Communications Unit, American University in Cairo
- Dr. Mervat el Rafie, Professor of Public Health, Cairo University
- Dr. Moukhtar el Tohamy, Dean of Communications, Cairo University
- Mr. Moustafa el Anany, Director of Health Programs, Television
- Dr. Moustafa Hamami, Vice Minister of M.O.H. for Primary Health Care and Family Health
- Dr. Nabil Younis, Gynecologist, Al Azhar
- Dr. Nadia Farah, Coordinator of Woman’s Health Book Project
- Ms. Nagwa Farag, UNICEF
- Dr. Naira el Akkad, Professor of Pediatrics, Al Azhar University
- Dr. Olfat Kamel, Professor of Public Health, Mansoura University
- Dr. Refeit Kamal, El Akhbar Newspaper
- Dr. Saadia Abd el Fatah, Prof. of Pediatrics, Ain Shams Univ.
- Dr. Said Ewaase, MOHP
- Dr. Salah Madkour, Director General for Communicable Diseases Control Department
- Ms. Samia Sadek, President of Egypt Television
- Dr. Samiha Gabriel, Director of Censorship, Television
- Dr. Samiha El Katsha, American University in Cairo
- Dr. Sarah Loza, SPAAC Research
- Dr. Shafika Salh Nasser, Professor of Public Health, Cairo University
- Dr. Sayed Hilal, Dean of Pharmacy, Cairo University
- Dr. Soad Hussein, Professor and Director of Nursing Institute, Assyut University
- Dr. Sobhy Moharram, UNICEF
- Ms. Susan Kline, John Snow, Inc. / NCDDP
- Dr. Youssef Adrees, Writer, Al Ahram Newspaper
CDC Staff
- Dr. Farag Elkamel, Founder & President
- Abdel Fattah Abdel Bary
- Dr. Fayka Bakr
- Nerman El-Hiny
- Walaa Amer
- Nadia Kamal
- Faten Hassouna
- Shaker Elkamel
- Tanya Kangas
- Ghada Sleem
Impact of the Sehettak Biddonia Project
Several pulications document the impact of this pioneering project. These are included elsewhere in this site:
https://elkamel.wordpress.com/2017/04/25/the-use-of-television-series-in-health-education/
https://elkamel.wordpress.com/2017/04/25/soap-operas-may-be-good-for-health/
https://idl-bnc-idrc.dspacedirect.org/bitstream/handle/10625/22955/109032.pdf?sequence=1
https://elkamel.wordpress.com/2017/04/25/idrc-health-the-soap-opera-version/